Overview
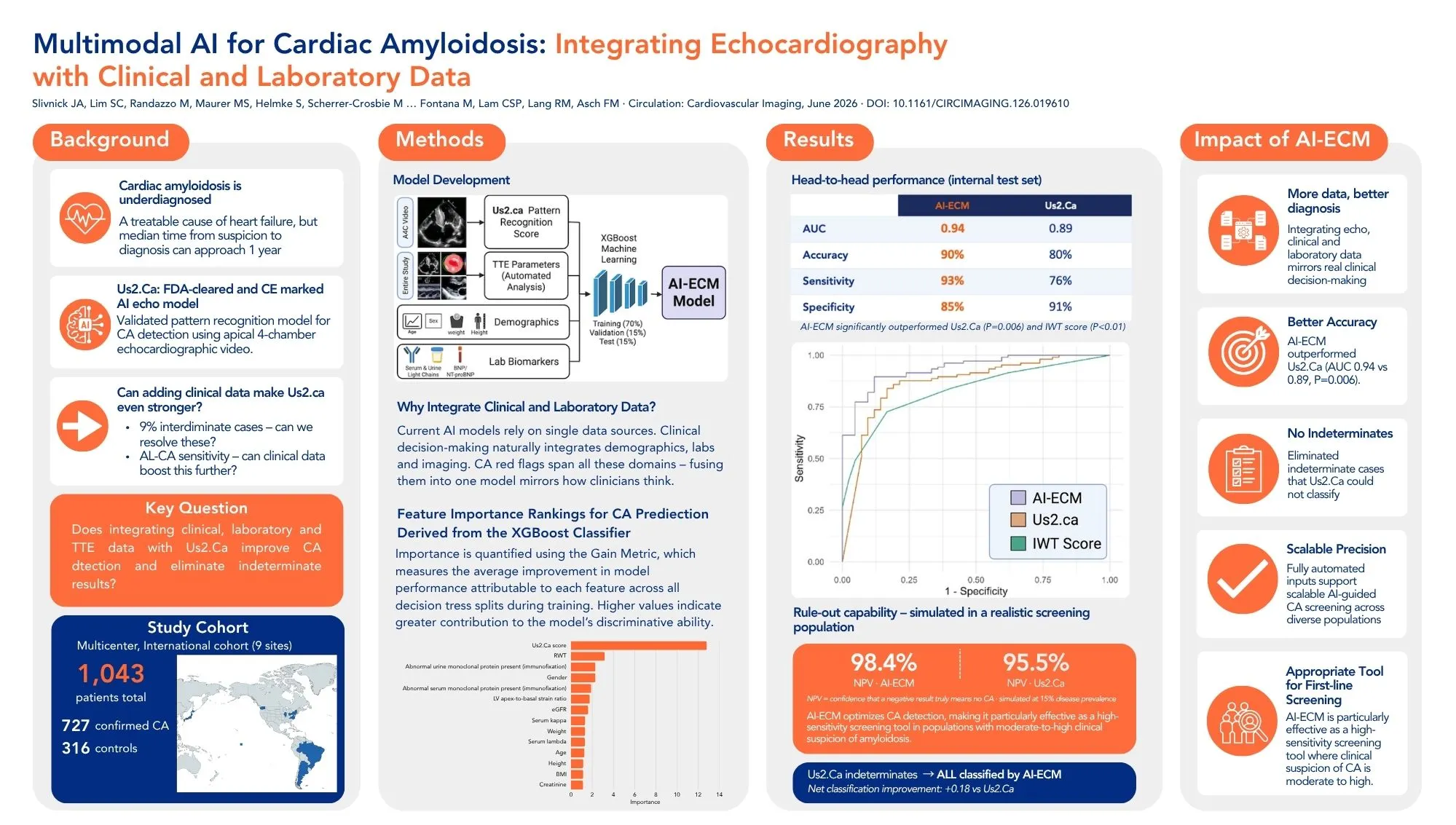
Cardiac amyloidosis is an underdiagnosed yet treatable cause of heart failure in which timely diagnosis is essential to access life-prolonging therapies. Despite growing awareness and the emergence of effective treatments for both major subtypes, diagnostic delays remain common, with median time from clinical suspicion to confirmed diagnosis approaching one year in real-world practice.
While AI-based tools using echocardiography, electrocardiography, and electronic health records have shown promise for cardiac amyloidosis detection, most rely on a single data source. This study asked whether combining the FDA-cleared Us2.Ca deep learning echocardiography model with routinely available clinical and laboratory data could further improve diagnostic performance, and whether doing so could eliminate the indeterminate classifications that limit deployment of TTE-only AI models in clinical practice.
Study Design
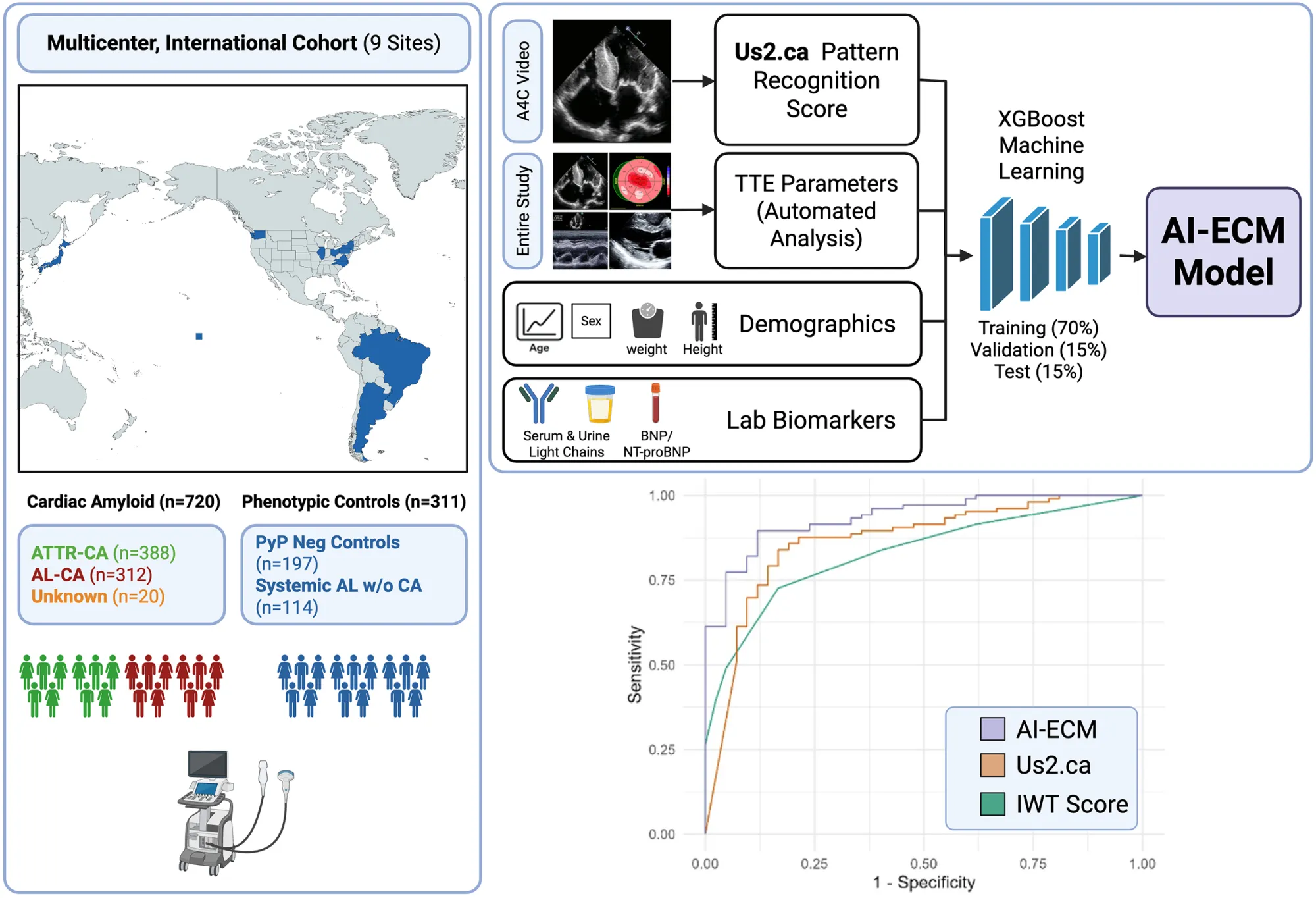
Researchers from nine academic medical centres across the United States, Japan, Brazil, Argentina, and the United Kingdom developed and validated a combined AI echo-clinical model (AI-ECM) using the Amyloidosis Imaging International Consortium, a large global multiethnic registry. The cohort included 727 patients with confirmed cardiac amyloidosis and 316 phenotypic controls, spanning both transthyretin and light chain subtypes.
The AI-ECM was built by integrating the probability score from Us2.Ca deep learning echocardiography model with routinely available parameters including relative wall thickness, LV apical-to-basal strain ratio, demographics, serum and urine light chain biomarkers, and renal function markers. All echocardiographic parameters were derived automatically using the Us2.ai FDA and CE-marked software pipeline, without manual input. The model was developed using XGBoost and evaluated against the TTE-only Us2.Ca model and established multiparametric echocardiographic scoring systems.
Key Results
The AI-ECM demonstrated superior performance compared to the Us2.Ca deep learning echocardiography model alone across all metrics.
The AI-ECM achieved an AUC of 0.94, accuracy of 90%, sensitivity of 93%, and specificity of 85%, compared to Us2.Ca alone which achieved an AUC of 0.89, accuracy of 80%, and sensitivity of 76% (p=0.006).
Critically, while the Us2.Ca model classified 9% of cases as indeterminate and therefore unable to be categorised, the AI-ECM produced a definitive classification for every patient. This is particularly significant given the clinical and prognostic harms associated with delayed or missed diagnoses.
Feature importance analysis identified the Us2.Ca score as the most influential input by a substantial margin, confirming that the deep learning echocardiographic model provides the primary diagnostic signal. Relative wall thickness, immunofixation findings, gender, and LV apical-to-basal strain ratio contributed additional incremental value.
The AI-ECM also improved sensitivity for light chain cardiac amyloidosis detection, a subtype where the echocardiography-only model performed least well, and maintained high accuracy across both cardiac amyloidosis subtypes and control groups.
Why This Matters
Cardiac amyloidosis is frequently missed at the point of initial echocardiographic assessment, when clinical suspicion may not yet be high and symptoms remain undifferentiated. Failure to detect it at this stage leads to delays in confirmatory testing and treatment initiation, with significant prognostic consequences.
This study demonstrates that by layering routinely available clinical and laboratory data onto the Us2.Ca echocardiographic AI model, it is possible to meaningfully improve screening sensitivity without additional imaging burden, while also eliminating the indeterminate classifications that have limited real-world deployment of TTE-only AI tools. All echocardiographic inputs were generated automatically by the Us2.ai platform, preserving the scalability and reproducibility of the approach.
The authors note that the data elements incorporated into the AI-ECM align with routine components of the early diagnostic evaluation for cardiac amyloidosis, making the model practical to deploy at the point of initial echocardiographic assessment in patients with suspected infiltrative cardiomyopathy.
Conclusion
This is the first study to fuse a deep learning TTE-based AI model with multimodal clinical, laboratory, and imaging biomarkers for cardiac amyloidosis detection. The resulting AI-ECM improves on the already high performance of Us2.Ca alone, achieves definitive classification in all cases, and represents a meaningful step toward scalable, AI-guided precision diagnostics for cardiac amyloidosis in diverse populations.
Hear from the Author: Dr. Jeremy Slivnick
Slivnick, J. A., Lim, S. C., Randazzo, M., Maurer, M. S., Helmke, S., Scherrer-Crosbie, M., Vakilpour, A., Zareba, K. M., Goyal, A., Cheng, R., Wakamatsu, N., Kitano, T., Takeuchi, M., Hotta, V. T., Vieira, M. L. C., Elissamburu, P., Ronderos, R. E., Prado, A., Koutroumpakis, E., Deswal, A.,…Asch, F. M.(2026). Multimodal Artificial Intelligence for Cardiac Amyloidosis Diagnosis: Integrating Echocardiography With Clinical and Laboratory Data for Improved Detection. Circulation: Cardiovascular Imaging. https://doi.org/10.1161/circimaging.126.019610