Overview
Early and accurate risk stratification after acute myocardial infarction (AMI) is critical for guiding therapy, personalising follow-up, and allocating clinical resources effectively. While conventional tools such as the GRACE score incorporate clinical and biochemical variables, they do not include echocardiographic parameters, despite echocardiography being routinely performed during AMI hospitalisation.
Beyond LVEF, novel echocardiographic markers of both systolic and diastolic function offer additional prognostic value but are not widely assessed in clinical practice due to time constraints, limited expertise, and interobserver variability. This study evaluated whether AI-derived echocardiographic parameters, generated automatically by Us2.ai, could provide incremental prognostic value on top of established clinical risk factors in a large, contemporary AMI cohort.
Study Design
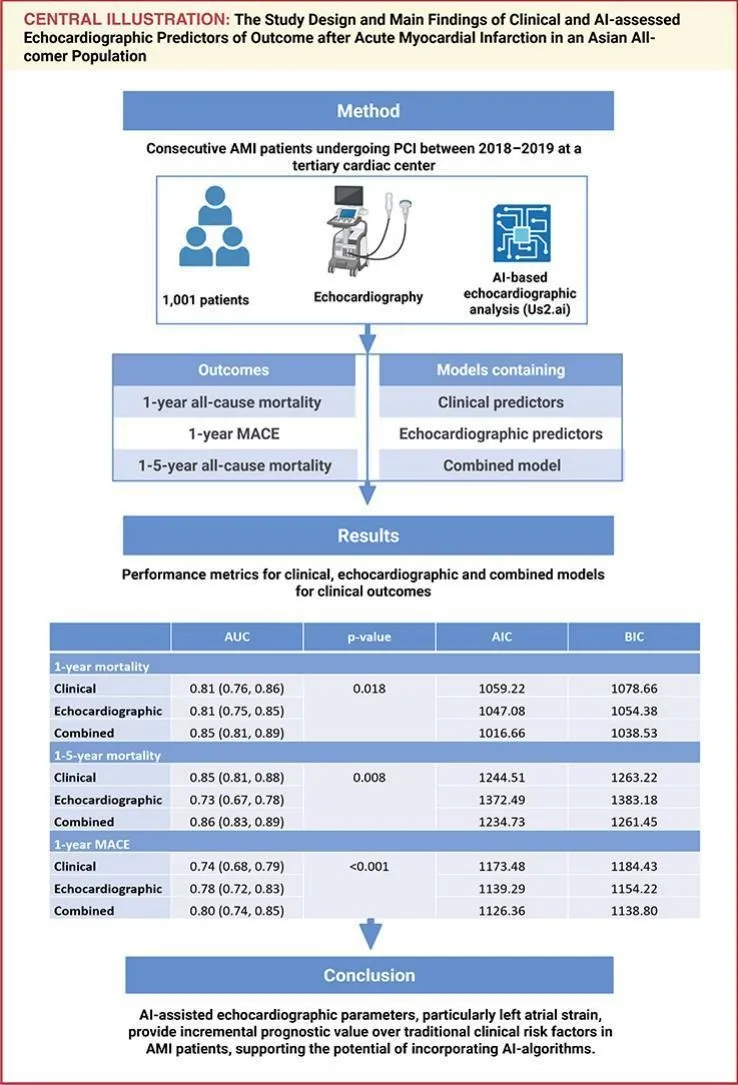
This retrospective study included 1,001 consecutive AMI patients undergoing percutaneous coronary intervention from the Singapore Cardiac Databank registry, a national prospective observational registry. The mean age was 64 years and 78.1% were male. Echocardiograms performed during the index hospitalisation were analysed using Us2.ai software, generating a comprehensive range of automated measurements covering ventricular and atrial volumes, wall thickness, LV mass, diastolic parameters, strain parameters, and aortic valve parameters.
Independent predictors of one-year all-cause mortality and major adverse cardiac events (MACE) were identified using Cox regression. Clinical, echocardiographic, and combined models were developed and compared across one-year and one-to-five-year follow-up periods.
Key Results
One-year Mortality:
- The combined model demonstrated superior discrimination compared to the clinical model alone (AUC 0.85 vs. 0.81, p=0.018)
- Independent AI-derived echocardiographic predictors included lower LVEF, lower LA reservoir strain, lower aortic valve area, lower LV mass, and higher aortic gradient
- The combined model also showed the most favourable Akaike and Bayesian Information Criterion values, indicating superior model fit
One-year MACE:
- The combined model significantly outperformed the clinical model (AUC 0.80 vs. 0.74, p<0.001)
- Independent echocardiographic predictors included lower LVEF, greater LV wall thickness, lower LV mass, greater LA area, lower LA reservoir strain, and lower aortic valve area
One-to-Five-Year Mortality:
- The combined model again achieved the highest discrimination (AUC 0.86 vs. 0.85 for the clinical model alone, p=0.008)
- Diastolic parameters including E/e' ratio and LA area emerged as independent echocardiographic predictors over this longer time horizon, suggesting diastolic remodelling plays an important role in longer-term post-AMI prognosis
LA Reservoir Strain:
- LA reservoir strain was an independent predictor of both mortality and MACE across time horizons, highlighting the prognostic importance of atrial function beyond conventional ventricular parameters
Why This Matters
Many of the echocardiographic parameters that proved independently prognostic in this study, including strain measurements and diastolic function indices, are not routinely assessed in all centres and can require additional time and expertise to measure reliably. Interobserver variability further limits their clinical utility when performed manually.
Us2.ai automates the measurement of these parameters accurately and reproducibly, making comprehensive echocardiographic risk stratification feasible without specialist input. This study demonstrates that AI-derived echocardiographic analysis can meaningfully augment conventional clinical risk scores in the post-AMI setting, with the potential to identify higher-risk patients who may benefit from more intensive monitoring or earlier therapeutic intervention.
The findings are particularly relevant for centres in lower-resource settings where advanced echocardiographic expertise may be limited, as AI-based analysis offers a route to standardised, comprehensive cardiac assessment at scale.
Conclusion
Combining AI-derived echocardiographic parameters with traditional clinical risk factors provides incremental prognostic value beyond either alone in patients following acute myocardial infarction. AI tools that automate complex echocardiographic assessments accurately and reproducibly have the potential to enhance post-AMI risk stratification in routine clinical practice.
Lenselink, C., Lau, Y. H., Huang, W., Ewe, S. H., Chiong, S. C., Ng, C. T., Ricken, K., Lipsic, E., Voors, A., Lam, C. S. P., Yeo, K. K., & Yap, J. (2026). Clinical and artificial intelligence assessed echocardiographic predictors of outcomes after acute myocardial infarction. International Journal of Cardiology, 460, 134638. https://doi.org/10.1016/j.ijcard.2026.134638