Heart failure most commonly comes to light only when a patient arrives at hospital in acute distress. Yet the conditions that cause it develop silently in the community, often over years, and frequently in people already known to primary care teams. The challenge has never been identifying who is at risk; it has been having a reliable, practical way to act on that risk before crisis strikes.
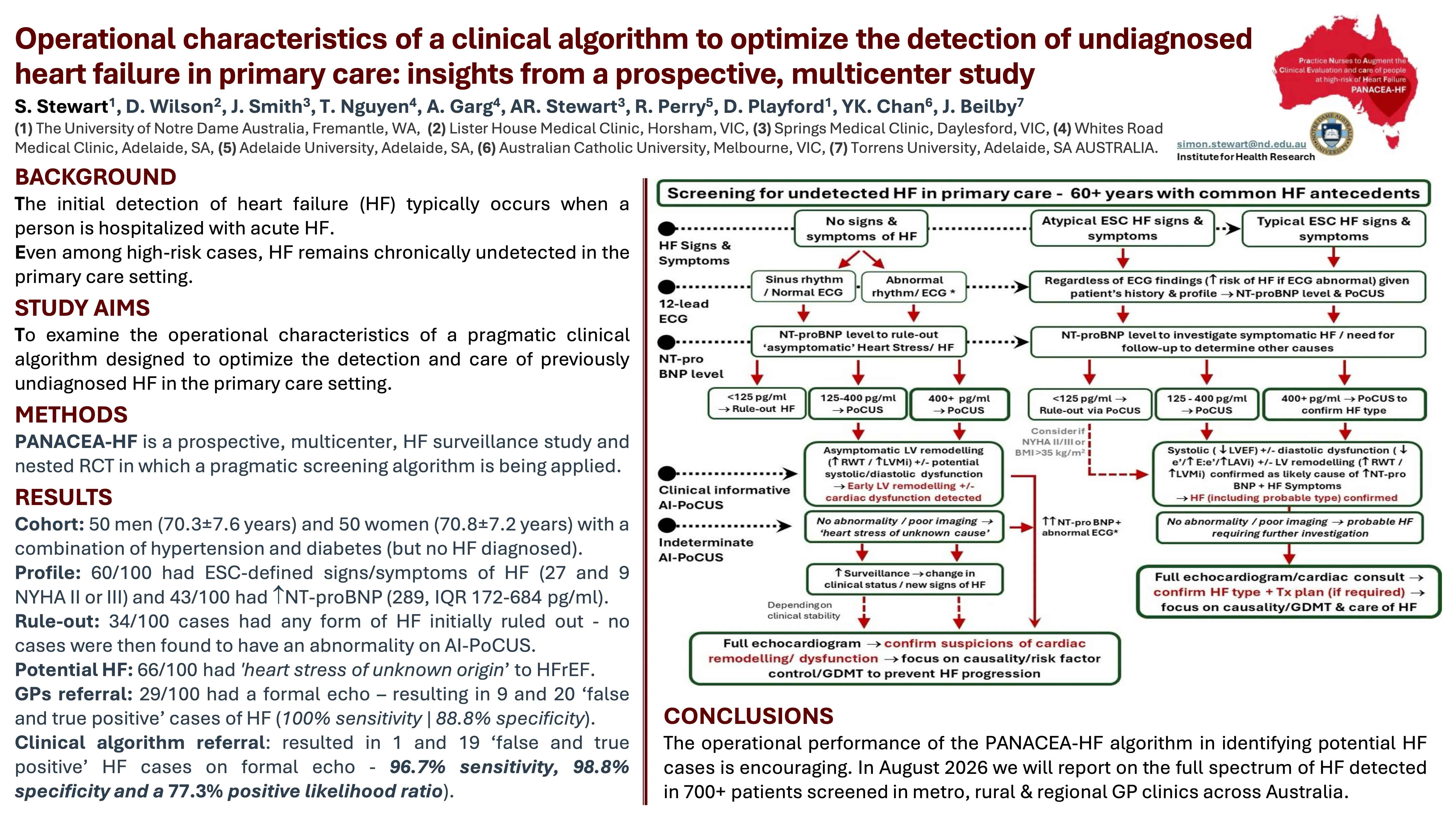
The PANACEA-HF study addresses this directly. Conducted across metropolitan and rural-remote primary care clinics in Australia, it is a prospective, pragmatic, multi-centre surveillance study and nested RCT applying a structured clinical algorithm to screen patients aged 60 and over with common heart failure antecedents. The algorithm integrates ESC-defined signs and symptoms, 12-lead ECG findings, NT-proBNP levels, and AI-mediated point-of-care ultrasound (AI-PoCUS) performed by practice nurses, producing a systematic pathway from initial profiling through to specialist referral or active surveillance.
In an initial cohort of 100 patients with hypertension and diabetes, the algorithm demonstrated a marked improvement over unaided GP clinical judgement. Where GPs referring on clinical grounds alone achieved 100% sensitivity but only 88.8% specificity (generating 9 unnecessary specialist referrals), the algorithm achieved 96.7% sensitivity and 98.8% specificity with just one false positive referral, and a positive likelihood ratio of 77.3%.
Key findings
- 34% of patients had HF reliably ruled out at initial profiling; none were found to have abnormalities on subsequent AI-PoCUS (100% sensitivity)
- GP-led referral: 100% sensitivity, 88.8% specificity, 9 false positive referrals from 29 total
- Algorithm-led referral: 96.7% sensitivity, 98.8% specificity, 1 false positive referral from 20 total
- Positive likelihood ratio of 77.3% (95% CI 11.0 to 543) for algorithm-guided referral
- 60% of patients had ESC-defined signs or symptoms of HF; 43% had elevated NT-proBNP on presentation
Implications
The PANACEA-HF clinical algorithm offers a structured, high-performing pathway to bring earlier heart failure detection into routine primary care, reducing unnecessary specialist burden while maintaining diagnostic rigour. For rural and regional settings where specialist resources are scarce, this kind of streamlined triage has particular value. Full results from 700+ screened patients across metro, rural, and regional GP clinics across Australia are expected in August 2026.