Article | SEP 12, 2025
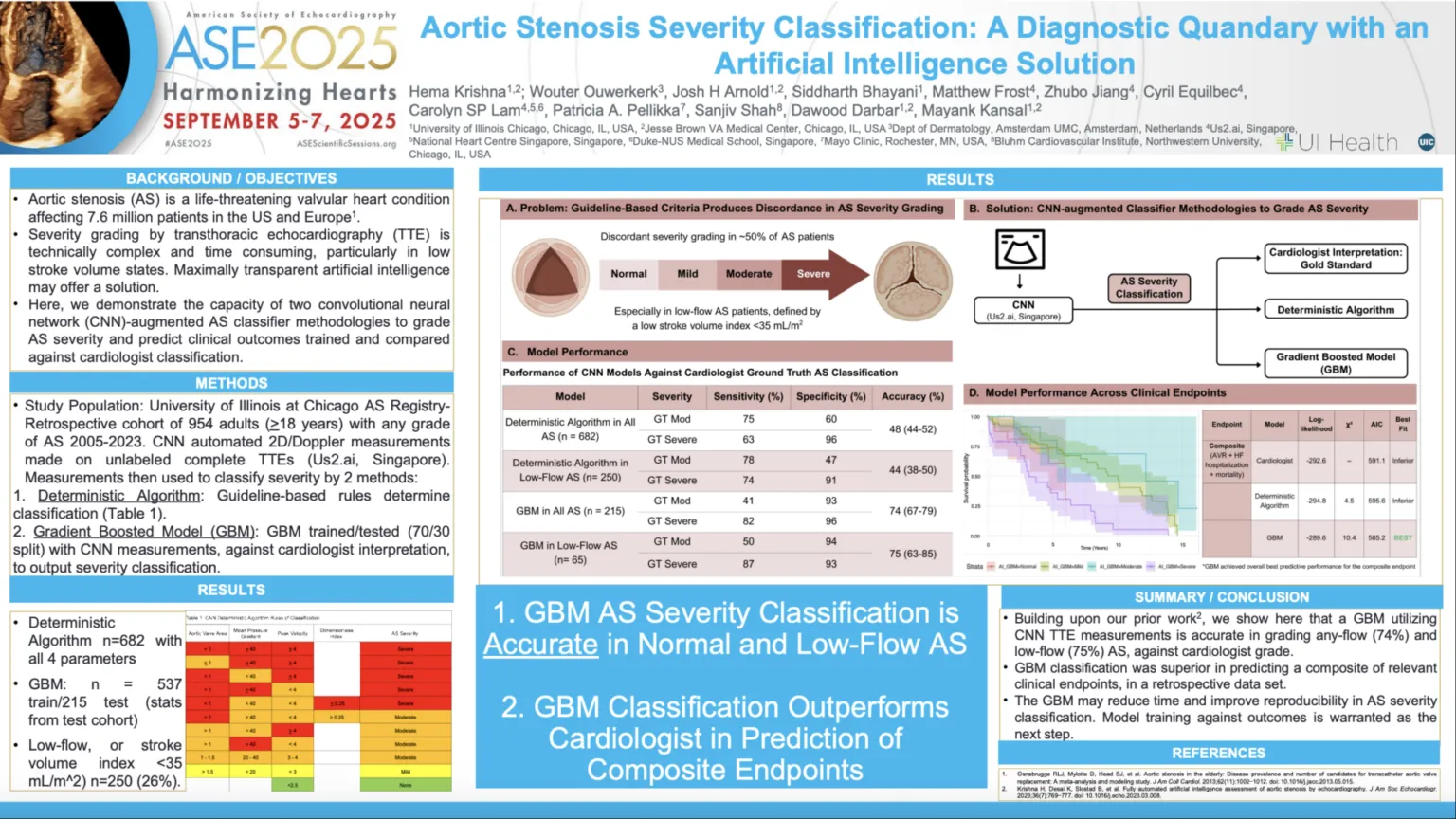
Aortic stenosis (AS) is a serious heart valve disease that is typically diagnosed using echocardiography. However, guideline-based classifications often produce discordant results and diagnostic uncertainty in up to half of patients, especially those with low-flow AS (stroke volume index ≤35 mL/m²).
In this study presented at ASE 2025, the authors explored two convolutional neural network (CNN)-augmented methods to grade AS severity and predict outcomes in a population enriched for low-flow AS. Echocardiograms from AS patients spanning 2005–2023 were included. Three classification approaches were compared:
- Cardiologist Classification: Ground truth based on the original cardiologist report.
- Deterministic Algorithm: Calculated AS severity using peak aortic jet velocity (Vmax), mean transvalvular pressure gradient (MG), aortic valve area by the continuity equation, and dimensionless index, with CNN-derived measurements (Us2.ai, Singapore).
- Gradient Boosted Model (GBM): Trained on CNN measurements against cardiologist classification to predict AS severity.
This study demonstrates that a novel CNN-augmented gradient boosted model (GBM) not only classifies aortic stenosis (AS) severity accurately using unlabeled echocardiograms but also outperforms cardiologists in predicting composite clinical endpoints. The technology may save time, improve reproducibility across readers and sites, and maintain strong performance even in patients with complex hemodynamic profiles.
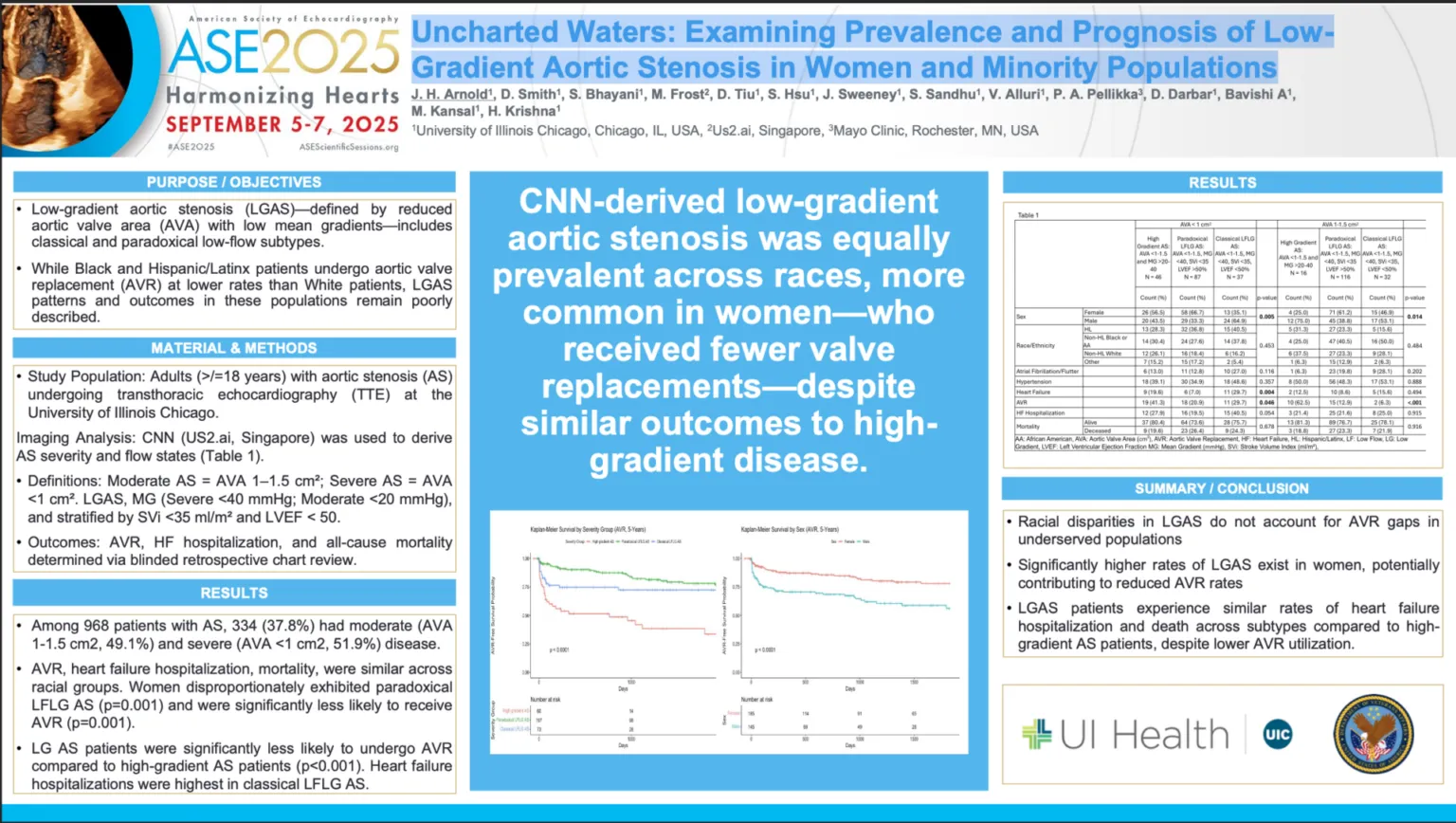
Low-gradient aortic stenosis (LGAS) is characterized by a narrow aortic valve area (AVA) with a low AV mean pressure gradient. Low AVmean pressure gradient and can be further divided into classical low-flow (LF) and paradoxical LF subtypes, depending on stroke volume index (SVi) and left ventricular ejection fraction (LVEF). While prior studies have shown that Black and Hispanic/Latinx patients undergo aortic valve replacement (AVR) at lower rates than White patients, little is known about the prevalence and outcomes of LGAS in minority-enriched populations.
In this study presented at ASE 2025, investigators analyzed 968 patients with AS at the University of Illinois Chicago using convolutional neural network (CNN)-derived echocardiographic measurements (Us2.ai, Singapore). Moderate and severe AS, as well as low-gradient states, were defined by CNN-derived hemodynamics, and outcomes were assessed through retrospective chart review.
Key Findings
- Prevalence: 37.8% of patients had moderate or severe AS;Rates of AVR, HF hospitalization, and mortality were similar across racial groups.
Prevalence:
- 37.8% of patients had moderate or severe AS;
- Rates of AVR, HF hospitalization, and mortality were similar across racial groups.
- Sex Differences: Women disproportionately exhibited paradoxical LFLG AS (p=0.001) and were significantly less likely to receive AVR (p=0.001).
- Clinical Outcomes: LGAS patients underwent AVR less frequently than high-gradient AS patients (p<0.001), despite experiencing comparable rates of HF hospitalization and death across subtypes. Classical LFLG AS was associated with the highest rates of HF hospitalization.
Conclusion
- Racial disparities in LGAS do not account for AVR gaps in underserved populations;
- Significantly higher rates of LGAS exist in women, potentially contributing to reduced AVR rates, and
- LGAS patients experience similar rates of heart failure hospitalization and death across subtypes compared to high-gradient AS patients, despite lower AVR utilization.
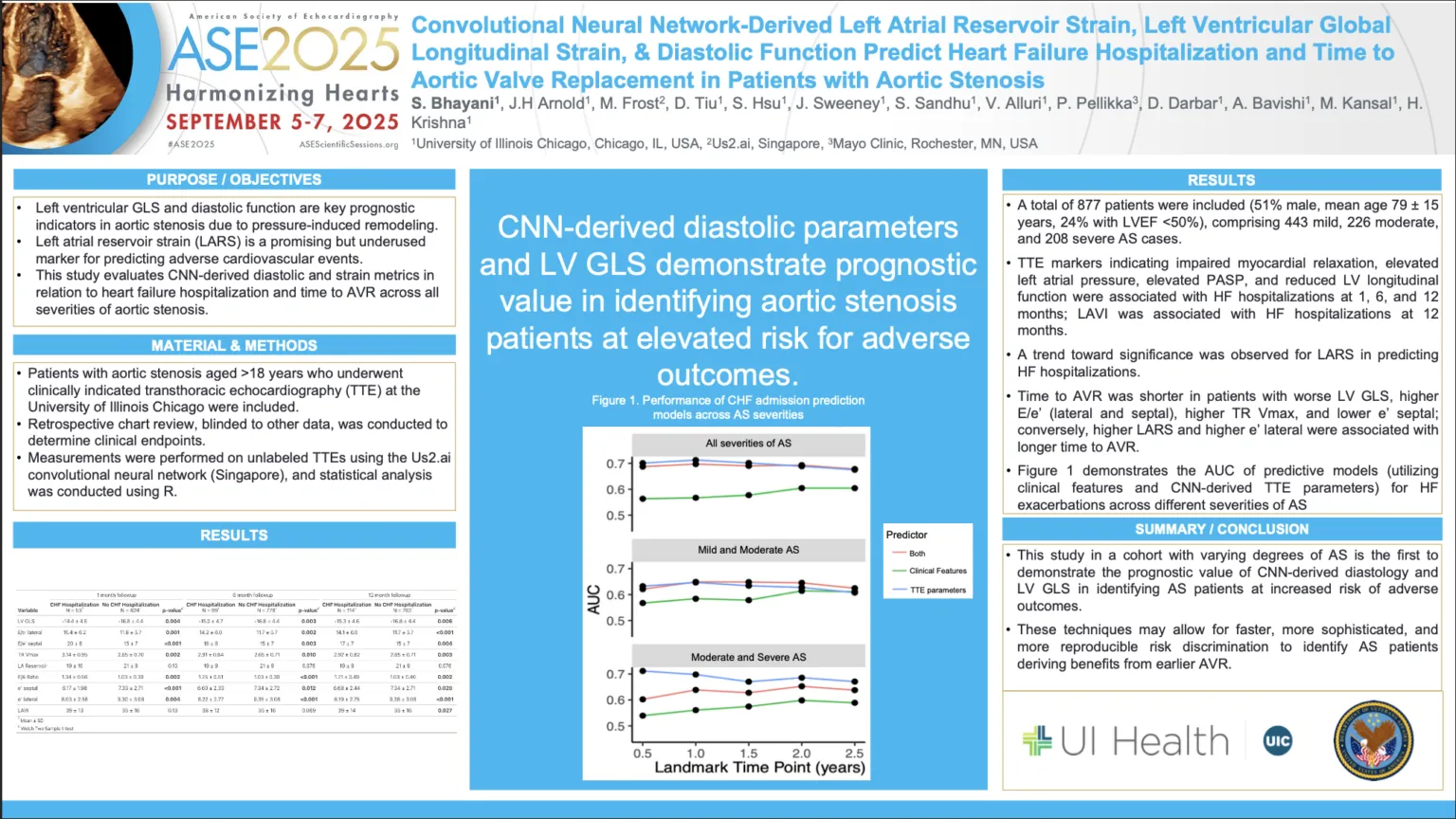
Aortic stenosis (AS) is a progressive valve disease associated with adverse cardiac remodeling and poor outcomes. While echocardiography is the standard tool for diagnosis and risk assessment, prognostic markers beyond traditional measures are needed to identify patients at highest risk for heart failure (HF) hospitalization or early aortic valve replacement (AVR).
In this study presented at ASE 2025, the authors investigated the role of convolutional neural network (CNN)-derived diastolic and strain parameters in predicting outcomes across the spectrum of AS severity. Echocardiograms from 877 patients (mild, moderate, and severe AS) were analyzed using Us2.ai’s automated platform, and results were correlated with clinical endpoints through retrospective chart review.
Key findings
- HF Hospitalization: Worsened diastolic function indices and impaired LV global longitudinal strain (GLS) were consistently associated with HF hospitalizations at 1, 6, and 12 months.
- Time to AVR: Patients with abnormal LV GLS, higher E/e’, and elevated pulmonary pressures underwent AVR sooner, while higher left atrial reservoir strain (LARS) predicted longer time to AVR.
This is the first study to demonstrate that AI-derived diastolic and strain parameters provide independent prognostic value in AS, offering faster, reproducible, and clinically meaningful risk stratification. These insights could help clinicians better identify patients most likely to benefit from earlier AVR.