Overview
Pre-operative cardiac assessment is critical for surgical safety, but time pressure and the skill demands of quantitative echocardiography make comprehensive evaluation difficult in routine peri-operative practice. This prospective multicentre study evaluated whether US2.ai could reliably automate that assessment, analysing 10 key echocardiographic parameters from a limited image sequence acquired by anaesthetists and comparing results against expert clinician measurements.
Study Design
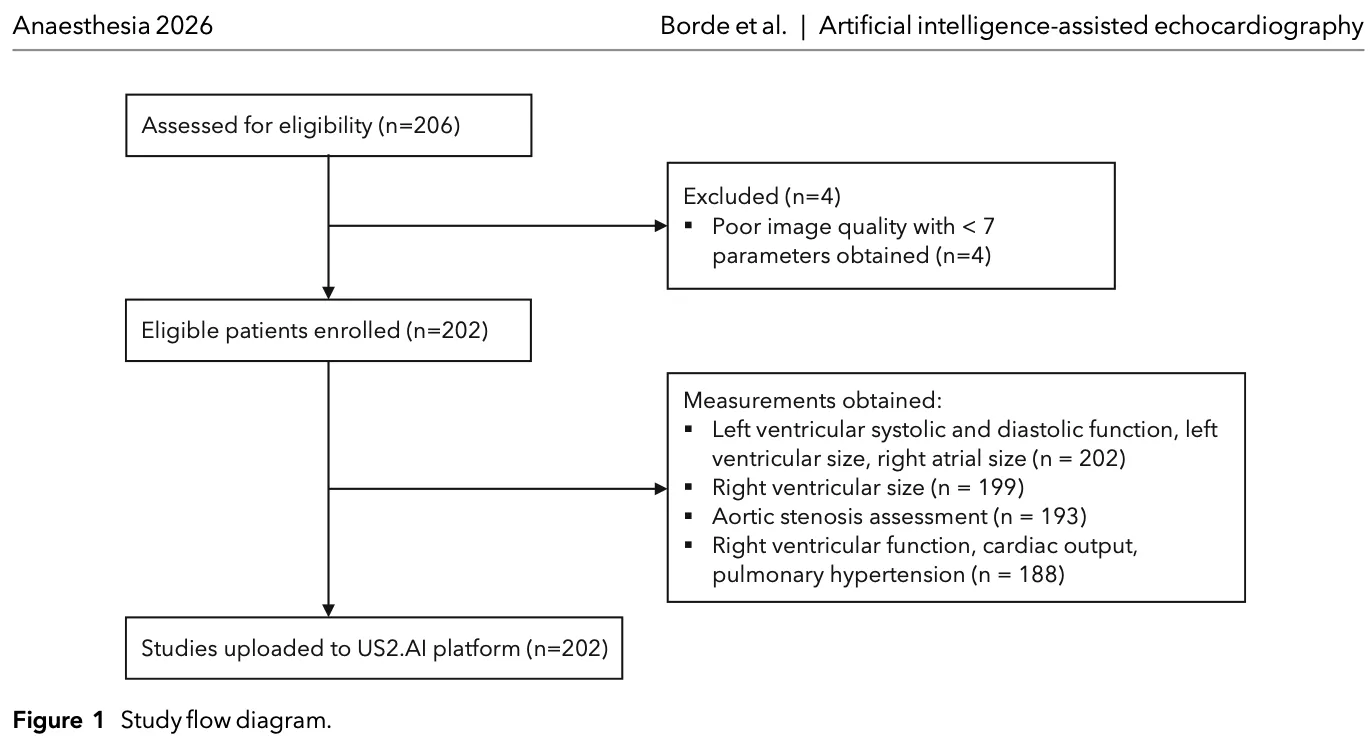
Conducted across five tertiary hospitals in India between March and May 2025, the study enrolled 202 adult patients scheduled for elective surgery across a range of surgical categories: cardiac, orthopaedic, laparoscopic, urological, gynaecological, and neurosurgical. Anaesthetists certified in echocardiography acquired a standardised 12-view transthoracic protocol. The same studies were independently analysed by expert clinicians and uploaded to the US2.ai cloud platform, which generated automated measurements and categorical classifications without any human input.
Key Findings
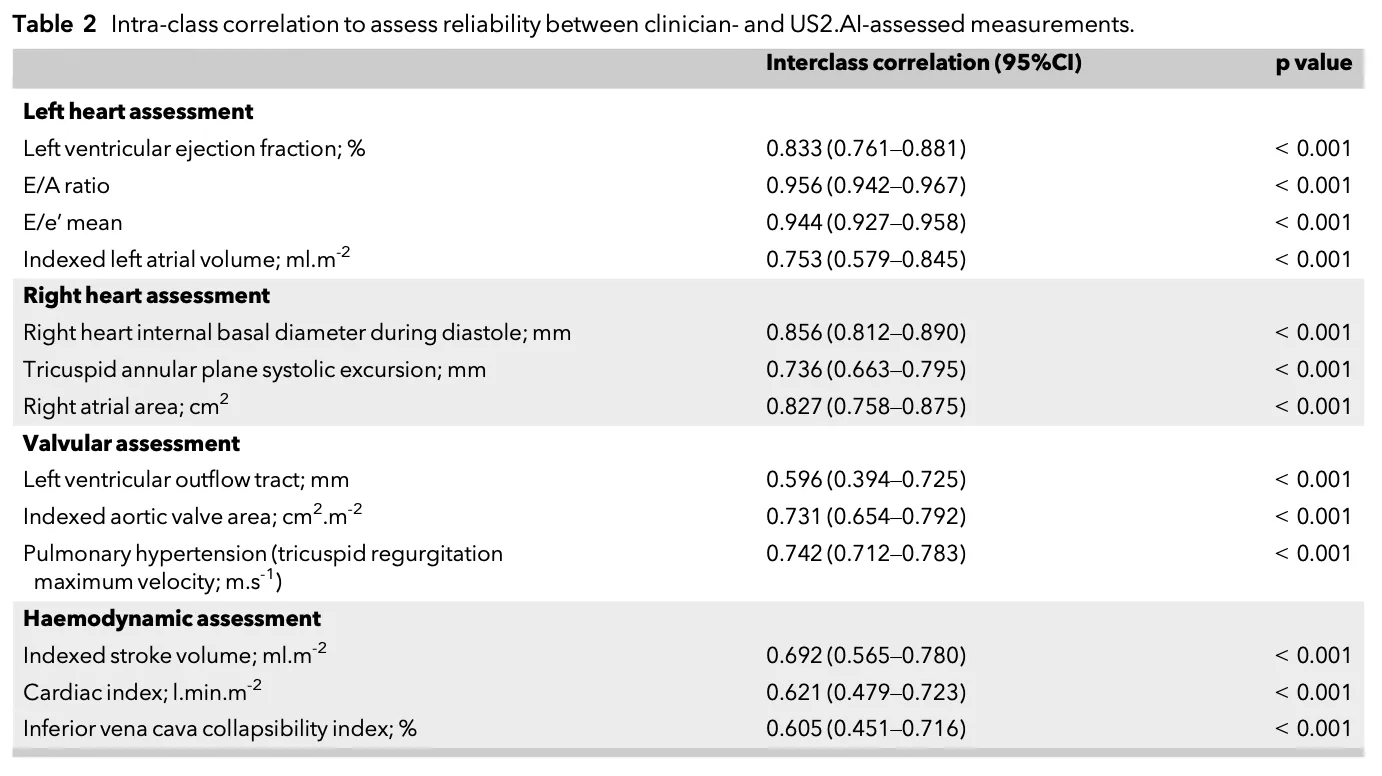
Agreement between US2.ai and clinician-derived measurements was good to excellent across most parameters, with intraclass correlation coefficient values ranging from 0.605 to 0.956 (p < 0.001 for all).
Highlights by cardiac domain:
Left Ventricular Function — LVEF showed strong correlation (r = 0.845, p < 0.001) with a mean difference of just −1.9%. US2.ai correctly classified LV systolic function in 91% of patients and LV diastolic dysfunction in 96% of patients.
Right Heart Assessment — Strong correlations were observed for right ventricular size (r = 0.860), right ventricular function (r = 0.743), and right atrial size (r = 0.842), all with minimal mean differences.
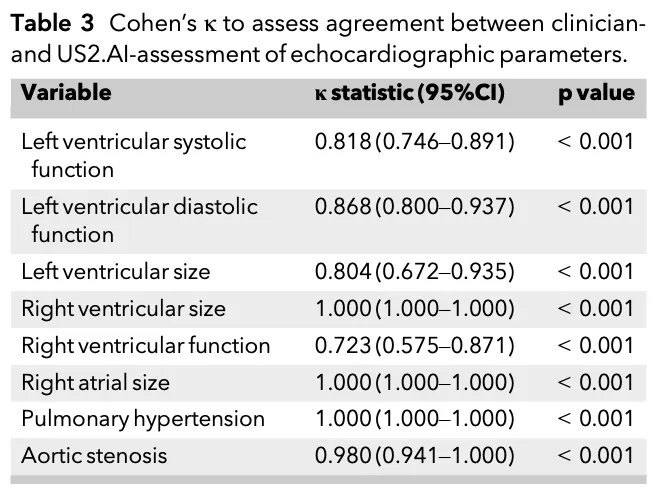
Critical Diagnoses — US2.ai identified 100% of patients with pulmonary hypertension (n = 10) and correctly classified all cases of severe aortic stenosis (n = 6), two conditions associated with markedly elevated peri-operative mortality.
Haemodynamic Parameters — Moderate agreement was demonstrated for IVC collapsibility (r = 0.641) and cardiac output (r = 0.675), with low mean bias.
Cohen's kappa for categorical classifications was statistically significant across all parameters (p < 0.001).
Why This Matters
Undetected cardiac pathology before surgery carries serious risk. Patients with severe aortic stenosis face a nearly 10% 30-day mortality rate following non-cardiac surgery, while those with pulmonary hypertension face up to four times higher adjusted mortality even in elective procedures. Accurate pre-operative identification of diastolic dysfunction, right ventricular impairment, and valvular disease enables anaesthetists to escalate monitoring, adjust management, and refer appropriately, decisions that depend on timely, quantitative data.
US2.ai delivers a comprehensive, automated echocardiographic report in under two minutes, without requiring expert input at point of care. This study demonstrates that, using a streamlined image acquisition protocol, anaesthetists can obtain actionable cardiac assessments that match expert clinician quality.
Conclusion
This is one of the first multicentre studies to validate AI-based comprehensive echocardiographic analysis across multiple parameters in a peri-operative setting. The findings support integration of US2.ai into pre-operative cardiac assessment workflows, with the potential to standardise quantitative echocardiography across centres regardless of local expertise.
Borde, D.P., Chidambaram, K., Jasapara, A., Madanaik, S.S., Joshi, S., Joshi, P., Apsingkar, P., Asegaonkar, B., Shetty, V., Elumalai, R., Chandrakumar, A., Dixit, A. and Swaminathan, M. (2026), Artificial intelligence-assisted peri-operative echocardiography: a multicentre observational study. Anaesthesia. https://doi.org/10.1111/anae.70235